

To date, several malignancies of the lymphoid lineage have been linked with microbial infection. Indeed, lymphomas have been associated with the bacteria Helicobacter pylori, and T-cell leukemia and Burkitt's lymphoma have long been known to be commonly caused by viral infections (human T-cell lymphotropic virus 1 and Epstein-Barr virus (EBV), respectively). However, metagenomics research in myeloid malignancies has primarily focused on the roles of gut flora rather than on the tumor site itself (blood and bone marrow).
Traditionally, human blood and bone marrow was considered to be normally sterile, and therefore microbiome analysis of these entities would only be performed when deleterious infection was suspected. However, evidence is now accumulating for a normal blood microbiome in healthy individuals. Given the growing number of established relationships in other malignancies between the microbiome at the tumor site and clinical characteristics, we hypothesized roles for the bone marrow microbiome in MDS patients. To this end, we extracted bacterial, fungal, and viral sequence from the bone marrow and blood of 640 MDS patients taken at diagnosis. Briefly, whole-genome sequencing (minimum coverage 100x) was performed on DNA extracted from each patient sample. Reads not aligning to the human genome were aligned to NCBI's database of known microbial reference genomes, and microbial species were assessed for presence and abundance in each sample.
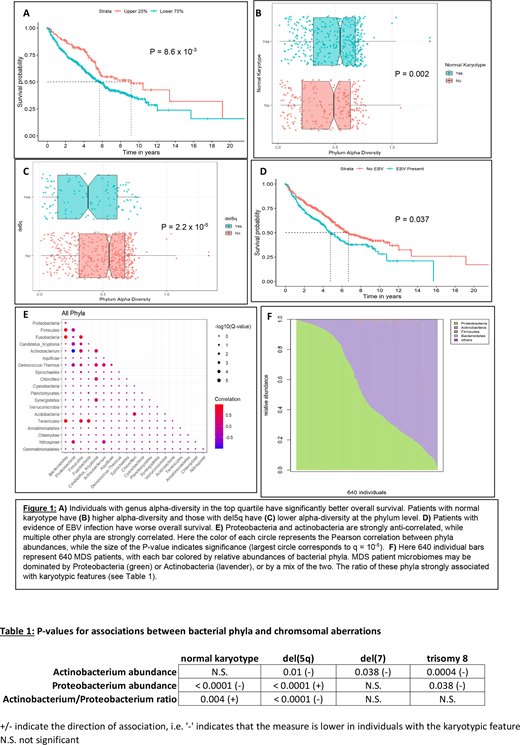
As expected, bacterial reads dominated, comprising 99.8% of all microbial reads, while viral reads were 2.73-fold as prevalent as fungal reads. We calculated microbial diversity (Shannon diversity index) on the genus and phylum levels for each patient. As has been reported in solid tumors, higher alpha-diversity is associated with favorable overall survival (age- and sex-adjusted P = 8.6 x 10-3; Figure 1A). Interestingly, individuals with normal karyotype had significantly higher alpha-diversity at the phylum level (Wilcoxon P = 0.002; Figure 1B), while those with deletion of chromosome 5q had significantly lower alpha-diversity (P = 2.2 x 10-5; Figure 1C).
Among viral infections, EBV (formally Human gammaherpesvirus 4) was the most common, with 192 patients (30%) harboring EBV DNA sequence. Human cytomegalovirus (HCMV; formally Human gammaherpesvirus 5) and Human betaherpesvirus 6 infections were also observed, in 23% and 2% of patients, respectively. EBV infection was associated with worse overall survival (age- and sex-adjusted P = 0.037; Figure 1D). There was also a substantial dose effect, with higher EBV levels corresponding to poorer outcomes (P = 1.96 x 10-6). Mining the paired-end DNA reads for human-viral chimeras, we found multiple instances of EBV integration into the patient genome, suggesting a possible mechanism for EBV infection impacting patient outcomes.
Bacterial composition was also analyzed, showing strong concordance between several pairs of phyla, suggesting synergy between these bacterial communities (Figure 1E). On the other hand, the Proteobacteria and Actinobacteria phyla were strongly discordant with one another (Figure 1E). Multiple studies have shown dominance of Proteobacteria in the circulating bacteriome of healthy individuals. In contrast, the MDS patients in our study showed a continuum between complete dominance of the Proteobacteria phylum and complete dominance of the Actinobacteria phylum (Figure 1F). Intriguingly, lower levels of Actinobacteria was strongly associated with the presence of various chromosomal aberrations, while the opposite was largely true for Proteobacterial abundance. As a result, the ratio of these two phyla abundances was strongly positively associated with normal karyotype and negatively associated with del(5q) (Table 1).
Overall, our study provides evidence for roles of the bone marrow microbiome in phenotypes and may even influence outcomes of patients with MDS. Further research is required to determine: a) whether microbial content is cause or consequence of patient characteristics, and b) what the mechanisms are for these microbiome-clinical associations.
Maciejewski:Alexion, BMS: Speakers Bureau; Novartis, Roche: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal